Yes—our care plans are evidence-informed and rigorously grounded in the best available research, clinical guidelines, and decades of proven real-world success, making them a powerful, reliable foundation for your evidence-based practice (EBP).
Understanding Evidence-Based Practice (EBP)
EBP, a standard in modern nursing since the 1990s (originating at McMaster University; Sackett et al., 1996), integrates three essential elements:
- The best available research evidence (from systematic reviews, RCTs, guidelines, etc.)
- Your clinical expertise and professional judgment
- Patient values, preferences, goals, culture, and circumstances
True EBP happens dynamically at the point of care, where you—the expert clinician—combine these elements to create individualized, effective care.
How CarePlans.com Strengthens Your EBP
Our library delivers a strong, dependable evidence foundation (the research leg of the EBP stool) so you can focus on what you do best: applying your expertise and tailoring care to each patient. Every plan is built from:
- Current, authoritative clinical practice guidelines (e.g., RNAO, NICE, AHRQ, USPSTF)
- Standards and recommendations from leading professional organizations (e.g., ANA, CMS)
- Peer-reviewed literature and high-quality sources
- Over 30 years of frontline clinical expertise and successful, field-tested implementations across diverse settings
This blend has empowered thousands of nurses to achieve better patient outcomes, streamline documentation, reduce errors, and save time—while meeting accreditation and quality standards.
We include full APA-style references for every key element, giving you complete transparency to review, appraise, and adapt sources as needed. Start with our plans as your trusted, up-to-date starting point, then layer in your clinical judgment and patient-specific needs for truly personalized, high-impact care.
In short: CarePlans.com doesn't replace EBP—it equips you to practice it more confidently and efficiently every day.
References
- American Nurses Association. (2015). Nursing: Scope and standards of practice (3rd ed.). American Nurses Association.
- Dang, D., Dearholt, S. L., Bissett, K., Ascenzi, J., & Whalen, M. (2022). Johns Hopkins evidence-based practice for nurses and healthcare professionals: Model and guidelines (4th ed.). Sigma Theta Tau International.
- Melnyk, B. M., & Fineout-Overholt, E. (2019). Evidence-based practice in nursing & healthcare: A guide to best practice (4th ed.). Wolters Kluwer.
- Registered Nurses’ Association of Ontario. (n.d.). Clinical practice guidelines. https://rnao.ca/bpg
- Sackett, D. L., Rosenberg, W. M. C., Gray, J. A. M., Haynes, R. B., & Richardson, W. S. (1996). Evidence based medicine: What it is and what it isn’t. BMJ, 312(7023), 71–72. https://doi.org/10.1136/bmj.312.7023.71
- U.S. Preventive Services Task Force. (n.d.). Recommendations. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation-topics
|
|
Yes! Careplans from the libary can be downloaded into Excel or Word, then modifiled. Careplans built in the client module can also be modified. Be sure to adapt outcomes and actions to align with your client’s individual situation.
|
|
Yes, all care plans are formatted for easy printing. Click on the “Print” button available on each care plan page.
|
|
Yes, but they should be adapted to meet the specific needs of your client and comply with your institution’s policies and guidelines.
|
|
Standardized care plans provide a great foundation, but they should always be individualized to the client’s specific needs. Tailoring care plans improves their effectiveness and ensures they are client-centered.
|
|
Absolutely yes!
Imagine a shared family office where multiple family members work together to manage information about certain projects. Here’s how it works:
- The "Account" is like the office itself. It’s a central hub where all the work is organized.
- "Members" are the family members (e.g., Mom, Dad, or a sibling) who have access to the office. Each member can walk into the office and work on the projects.
- "Clients" are the projects (e.g., a grocery list, vacation plans, or bills) that the family members are managing together.
How They Connect
The relationships work like this:
- Multiple family members (Members) can use the same office (Account) to access the same projects (Clients). For example, both Mom and Dad can access the grocery list or vacation plans in the office.
- The office (Account) connects everyone, so all authorized family members can see and work on the same set of projects without needing separate offices.
This setup allows multiple people (Members) to share access to the same information (Clients) through one central system (Account), making collaboration easy and organized.
|
|
Yes! The vast majority of careplans include rationales for outcomes as well as actions.
|
|
No, this site does not include NANDA-I Nursing Diagnoses. While we previously licensed the NANDA-I library, we discontinued this for two main reasons:
- The majority of our members did not utilize the NANDA-I content.
- The NANDA-I library was available for free at https://nandadiagnoses.com.
Given this accessibility, we determined that maintaining a recurring license fee for data readily available online was not a sustainable choice for our platform.
Update 3/23/25: The above URL was taken down and now redirects to the NANDA-I website.
|
|
Care plans serve as a communication tool among the interdisciplinary team, ensuring all healthcare professionals (nurses, physicians, therapists, social workers) are aligned in the client’s care.
|
|
EHRs have streamlined care planning by providing templates, real-time updates, and easy access to client data. However, nurses must ensure that care plans remain individualized rather than relying solely on pre-built templates.
|
|
Log-in and go to your "My Account" page. There are two ways to access the "My Account" page. There is a menu option in the left
panel labled "My Account". There should also be a link in the top right corner of the screen.

Once you're in the "My Account" section. Click the menu option for "Account Settings"
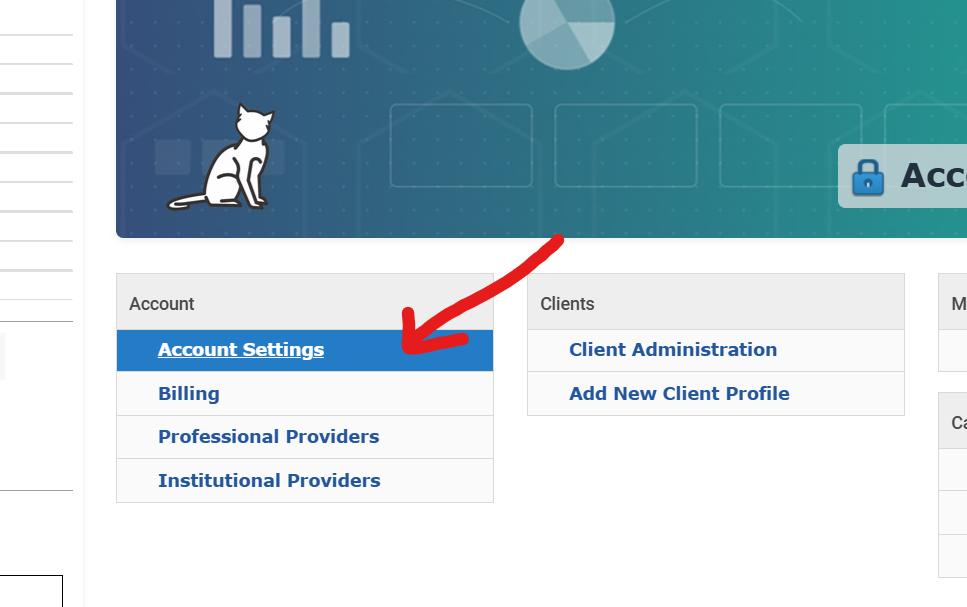
In the "Account Settings" Page, you should see an option on the left menu bar labeled "Cancel Account". Once you click that option,
you should access the "Cancel Account" page. Please select a reason for cancelling from the drop-down select box, and give us some feedback
as to how we might improve the site! For a short-cut, click HERE
|
|
Care plans typically follow this structure:
- Assessment: Gather client data (history, physical exam, lab results, etc.).
- Issues Identification: Identify the client's health problems or nursing issues.
- Outcomes: Define what improvement or changes are expected in the client’s condition.
- Actions: List nursing interventions that will help achieve the outcomes.
- Evaluation: Assess whether the outcomes were met and adjust the plan as needed.
|
|
Many EHRs allow importing documents in specific formats. You can download the care plan as a PDF, Word document, or plain text and upload it into your EHR system. For specific instructions, consult your EHR software’s user guide.
|
|
To evaluate effectiveness:
- Compare the client’s current status with the defined outcomes.
- Assess whether the actions were implemented as planned.
- Determine if adjustments are needed to improve results.
|
|
Use the search bar on the CarePlan Library page to type the condition you’re looking for (e.g., diabetes, hypertension).
|
|
Writing a care plan involves these steps: 1. Identify the client’s issues (e.g., ineffective airway clearance). 2. Determine measurable outcomes (e.g., client will maintain oxygen saturation above 95% within 48 hours). 3. Develop specific, evidence-based actions (e.g., administer oxygen as prescribed, monitor respiratory rate hourly). 4. Evaluate the outcomes and revise as necessary.
|
|
Yes, the care plan database is available for purchase in SQL Server format for $8,000. Please contact info@careplans.com for more information.
|
|
Yes. CarePlans.com membership is very inexpensive and can be cancelled anytime.
|
|
Common challenges include:
- Lack of detailed assessment data: A strong care plan is based on thorough assessment.
- Unclear or unrealistic outcomes: Outcomes should be SMART (Specific, Measurable, Achievable, Relevant, Time-bound).
- Generic actions: Actions should be specific to the client’s condition rather than vague or general.
- Failure to evaluate and update: Care plans should be dynamic, adjusting as the client’s condition changes.
|
|
If outcomes are not met:
- Reassess the client’s condition for any new issues.
- Modify or adjust actions as needed.
- Consider if the outcomes were realistic given the client’s condition.
|
|
A care plan is a structured, individualized approach to providing healthcare that outlines a client’s needs, desired outcomes, and the actions required to achieve those outcomes. It serves as a communication tool among healthcare providers, clients, and families.
|
|
PDPM and Its Relation to MDS in Long-Term Care
PDPM, or the Patient-Driven Payment Model, is a reimbursement system implemented by the Centers for Medicare & Medicaid Services (CMS) for skilled nursing facilities (SNFs) under Medicare Part A, effective October 1, 2019. It replaced the Resource Utilization Group (RUG-IV) system and ties payments to patient characteristics and care needs, as documented in the Minimum Data Set (MDS) assessments.
Key Points about PDPM and MDS
- Purpose of PDPM:
- Aligns Medicare payments with clinical complexity and resident needs, not service volume (e.g., therapy minutes).
- Improves payment accuracy, reduces administrative burden, and encourages holistic care.
- Role of MDS in PDPM:
- The MDS is a standardized tool collecting clinical data on diagnoses, functional status, cognitive status, and care needs.
- MDS data drives reimbursement by determining case-mix classifications for payment components.
- PDPM Components:
PDPM calculates reimbursement based on six components, each with case-mix groups derived from MDS data:
- Physical Therapy (PT): Based on primary diagnosis, functional status (MDS Section GG), and cognitive status.
- Occupational Therapy (OT): Similar to PT, using diagnosis, functional status, and cognitive status.
- Speech-Language Pathology (SLP): Based on swallowing disorders, speech/language deficits, cognitive impairment, and diagnoses (e.g., stroke).
- Nursing: Determined by clinical conditions, functional status, and nursing care needs (e.g., IV medications, wounds).
- Non-Therapy Ancillary (NTA): Accounts for high-cost ancillary services (e.g., medications, supplies) based on comorbidities.
- Non-Case-Mix: Fixed component for facility overhead, not tied to MDS clinical data.
- MDS Assessments Under PDPM:
- 5-Day Assessment: Initial MDS within 8 days of Medicare Part A stay, sets payment rate.
- Interim Payment Assessment (IPA): Optional if resident’s condition changes significantly, adjusting payment.
- Discharge Assessment: Captures status at end of Medicare Part A stay.
- Accurate coding of diagnoses (ICD-10), functional scores (Section GG), and comorbidities (Section I) is critical.
набирай - Impact on Long-Term Care:
- Clinical Focus: Incentivizes focus on clinical needs and comorbidities, not therapy minutes.
- Documentation: Requires precise MDS coding to avoid underpayment or audit risks.
- Interdisciplinary Approach: Encourages collaboration among nursing, therapy, and medical staff.
- Key MDS Sections for PDPM:
- Section GG: Functional abilities (mobility, self-care) influence PT, OT, and nursing.
- Section I: Diagnoses and comorbidities drive PT, OT, SLP, and NTA rates.
- Section O: Special treatments (e.g., ventilator care, IV medications) impact nursing and NTA.
- Section C and B: Cognitive status (e.g., BIMS) affects SLP and other components.
Summary
PDPM uses MDS data to classify residents into case-mix groups determining Medicare Part A reimbursement for SNFs. The MDS captures clinical and functional data reflecting care needs. Accurate, timely, and comprehensive MDS assessments ensure appropriate payment and compliance.
|
|
A care plan is a comprehensive document that includes multiple aspects of client care, while a nursing diagnosis (better referred to as a nursing issue in the CAT system) is a specific problem identified as part of the care plan. Care plans include outcomes and actions tailored to address these issues.
|
|
Care plans should be grounded in evidence-based practice, meaning actions should be based on the latest research and clinical guidelines. This enhances the quality and effectiveness of client care.
|
|
Outcomes are the desired results or goals for the client (e.g., improved mobility). Actions are the steps taken to achieve those outcomes (e.g., assist with range-of-motion exercises twice daily).
|
|
A care plan is typically developed by healthcare professionals such as nurses, doctors, or case managers, often in collaboration with the client and their family. In some cases, interdisciplinary teams contribute to its development.
|
|
Care plans ensure continuity of care, promote collaboration among healthcare providers, and keep care focused on the client’s specific needs and outcomes. They help identify priorities and streamline treatment.
|
|
 | Loading… |
|